The pandemic appears to have caused unusual behavior by some common viruses. Especially those of respiratory transmission.
In the 2020-2021 season there were practically no cases of the flu. The 2021-2022 season began with low records but, in an unusual way, it has been stretching during the spring until practically reaching the summer. Interestingly, a classic lineage of the flu virus (Influenza B Yamagata) seems to have disappeared. Or at least he hasn’t isolated himself in recent months.
The other “great” respiratory virus, the respiratory syncytial virus (RSV), significantly reduced its incidence in 2020 and 2021. But it has also maintained strange behavior, with outbreaks in summer and outside its usual season.
Fewer colds, more tuberculosis and monkeypox
Seasonal coronaviruses, which cause colds, have also reduced their presence in recent years. The rhinoviruses, however, which cause the common cold, seem to have remained stable or even increased during the pandemic. A fact that suggests that they can use different transmission routes than other respiratory viruses. We can even conjecture that they are less sensitive to mitigation measures and social distance.
In the case of tuberculosis (a bacillus), worldwide and after a decade of continuous decline, deaths have risen to 1.5 million, even with a reduction in reported cases. However, in some places, like the state of washingtonvery large outbreaks have been reported during the pandemic.
Beyond respiratory viruses, this year we have been surprised by adenoviruses, associated with outbreaks of acute childhood hepatitis of unknown cause (without causality being clearly established). Fortunately, in United Kingdom In the US and Europe, the cases seem to be remitting in recent weeks, without an apparent explanation for the decrease.
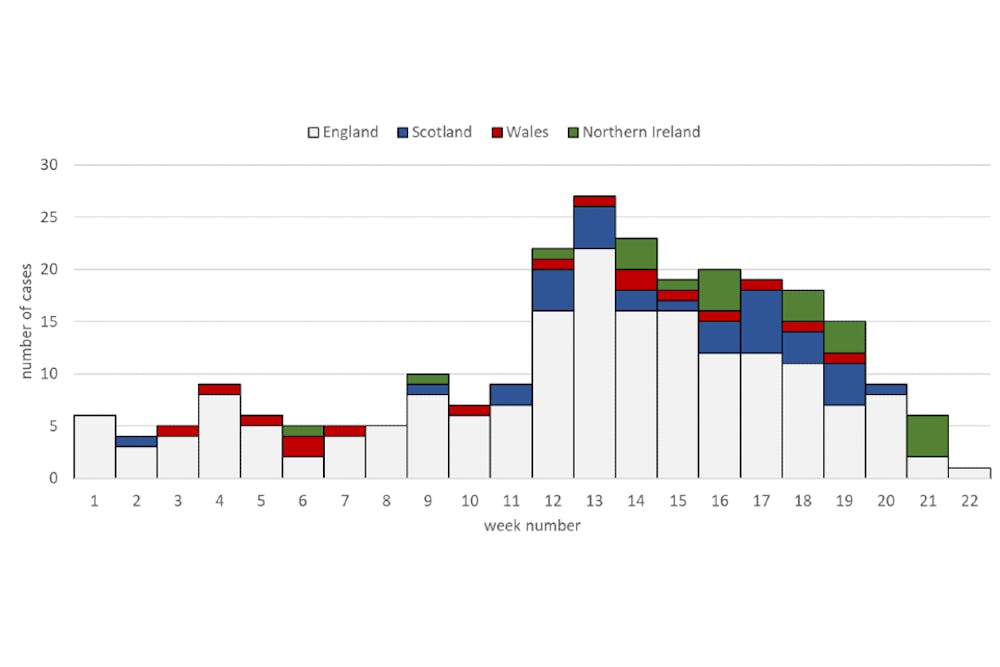
UK Health Security Agency, 2022
Obviously, we have also been alarmed by the monkeypox virus (monkey pox). with multiple outbreaks outside its endemic area in West Africa, and with apparently unusual population groups and routes of transmission for this virus.
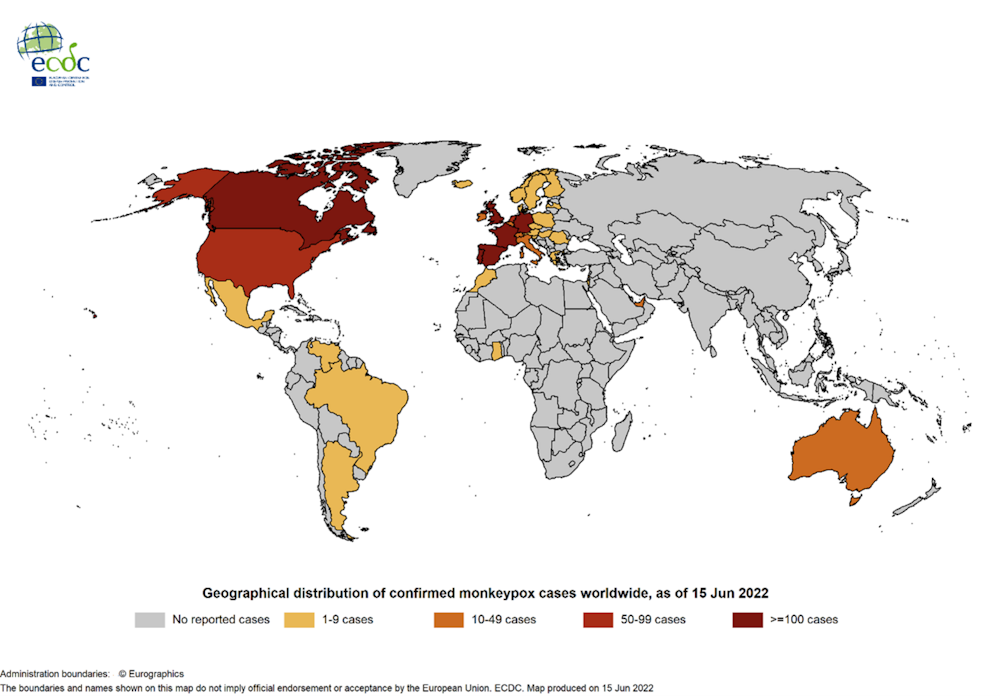
European Center for Disease Prevention and Control
What has changed with the pandemic?
Changes in virus behavior have several possible explanations. The first, obvious one, is that many of the measures adopted to mitigate the transmission of SARS-CoV-2 also hindered the transmission of other viruses.
The measures of social distance, masks, prohibition of massive events, limitations on leisure and work trips (including intercontinental ones), reduction of capacity and ventilation of interior spaces, hand washing and some other seem sufficient to explain the reduction in infections. of respiratory and contact transmission in the pandemic period.
Another explanation – speculative, and derived from the previous one – would be that the microscopic rivals of SARS-CoV-2 have evolved to improve their adaptation to the selective pressure caused by mitigation measures. Evolutionarily, strains capable of better competing with SARS-CoV-2 would be selected.
More plausible it seems that the lack of recent exposure to some viruses has made us more susceptible when we abandon mitigation measures. Or that less exposure makes it difficult for us to develop better immune responses once infected and we see more serious cases of the same viruses. In this case, the viruses would not have changed as much as we did.
A final explanation would simply be that our epidemiological surveillance systems (and our media and our subjective perception of risks) have become hypersensitive to everything that sounds like a virus. If we are permanently alert, we detect more threats. We will even interpret as threats things that did not seem so to us before.
The more you look, the more you see
The recorded incidence of many health problems is highly sensitive to the type and intensity of screening activities. We talk about surveillance bias (surveillance bias) when these health problems are sought with a different intensity between populations, over time, or according to the care environment and the characteristics of the patient.
The “surveillance bias” causes us to find more cases when there is not so much real change in incidence as differences in detection intensity: The more you look, the more you see. The case of tuberculosis is possibly the reverse example: we reduced detection during the pandemic and now we find the cases that we had missed.
The impact of this bias has been discussed in other public health crises. For example, after the Chernobyl nuclear accident, a increase in thyroid cancer in nearby areas. It was probably real but it is also likely that the search for cancers after the accident overestimate the size of the increment.
There is also the case of the increases in Creutzfeldt-Jakob disease associated with the “mad cow” crisis (bovine spongiform encephalopathy) that could be explained, in large part, by the higher number of autopsies looking for this disease in older people.
A close relative of the “surveillance bias” is the so-called “verification bias” (ascertainment bias). It occurs when detection is differential between population groups because their exposure or risk is different.
For example, it is more likely to detect cases of monkeypox among men who have sex with men (MSM) than among heterosexuals. Simply because when faced with the same symptoms, some will go to health services more than others. And because, additionally, clinicians will look for the disease more among MSM people than among heterosexuals.
The same explanation for all viruses?
It is possible that a single cause of those previously mentioned does not explain the apparent strange behavior of very different viruses and with different transmission routes. In some cases we will be more susceptible after two years without exposure. In others, we will be overdetecting. Even both things at the same time, to a greater or lesser extent.
It is even possible that in some of the examples, such as monkeypox or acute childhood hepatitis, we are now detecting cases that had been circulating for some time, perhaps years, under the radar of our surveillance systems.
And it is precisely in that basket, in surveillance, that we have to put our efforts. Rather than unsettle us with speculation about the “mental health” of microscopic beings, reinforcing our epidemiological surveillance systems seems the best way to address the future of our relationship with viruses.
A future that, moreover, through climate change and globalization, seems uncertain and complicated.
Salvador PeiroResearcher, Health Services Research Area, FISABIO PUBLIC HEALTH, Phisabio
This article was originally published on The Conversation. read the original.